Protocol for Medication Abortion Using Mifepristone and Misoprostol
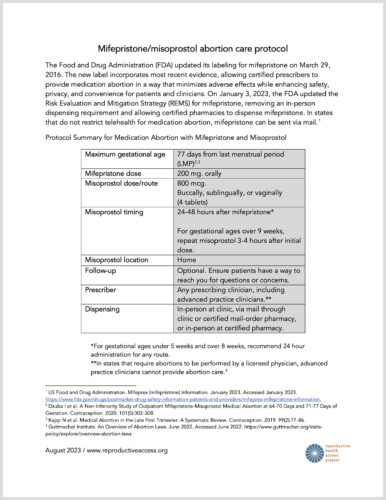 This is a protocol for providing a medication abortion using mifepristone and misoprostol. The protocol includes guidance on providing medication abortion without ultrasound.
This is a protocol for providing a medication abortion using mifepristone and misoprostol. The protocol includes guidance on providing medication abortion without ultrasound.
You can Support Project Access today!
This is a protocol for providing a medication abortion using mifepristone and misoprostol. The protocol includes guidance on providing medication abortion without ultrasound.
This bi-monthly clinical e-newsletter highlights evidenced-based best practices in abortion and miscarriage care
Apr 18
