Aug 14

Help Us Protect Access to Sexual and Reproductive Health Care Today!

On July 13th, a federal judge in Maryland suspended a FDA rule that requires people seeking medication abortion care to visit a hospital or clinic in-person to obtain mifepristone, one of two medications used in a medication abortion. This ruling allows providers around the country to mail or directly deliver mifepristone to patients during the pandemic. RHAP celebrates this ruling as essential to ensuring abortion access for all during this public health emergency, especially for Black, Indigenous, People of Color (BIPOC), people living in rural areas, and people living in poverty, who are most heavily impacted by attempts to restrict abortion care.
The FDA’s Risk Evaluation and Mitigation Strategies (REMS) on mifepristone, like requiring in-clinic patient visits, are medically unnecessary and pose as obstacles to abortion care access. We applaud the ACLU, NYSAFP, and all the activists who made this ruling possible. However, we know the fight to expand access to mifepristone is far from over. The REMS restrictions on mifepristone need to be suspended permanently and must also be lifted for people seeking to manage their early pregnancy loss.
For more information on reproductive care during the COVID-19 pandemic and guidance on how to provide medication abortion via telemedicine, check out https://www.reproductiveaccess.org/covid19/, our resources supporting reproductive health care providers during this time.
This article was written by our summer intern, Vishu Chandrasekhar. Vishu is supported by the Civil Liberties and Public Policy Program.
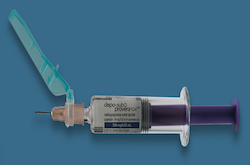
Depot medroxyprogesterone acetate (DMPA), often referred to by the brand name, Depo Provera, or “the depo shot,” is birth control that is administered as an injection every three months to prevent pregnancy. The most common form is an intramuscular injection, which usually involves going to a health care provider — like a doctor, nurse, or pharmacist — to receive it. While coming to the clinic to receive birth control is typically acceptable for some patients, accessing birth control in an in-clinic setting during the COVID-19 pandemic can put patients and health care workers at risk of exposure to the virus unnecessarily. There is, however, a self-administered version of the depo shot called DMPA-SC (SC means subcutaneous, or under the skin), in which clinicians send a prescription to patients’ local pharmacies every three months where they can administer the shot at home. DMPA-SC helps address the barriers and risks of accessing contraception every three months through an in-clinic visit. Unfortunately, not all insurance companies cover DMPA-SC, some pharmacies do not carry it, and some pharmacists will not dispense it without an additional note for clinician-supervision. Despite ample evidence in the US and globally that self-administration is just as safe and efficacious as clinic-administered, the FDA label as clinic-only administration most likely contributes to these obstacles to access. These barriers are unacceptable, especially during a pandemic when improved access to DMPA-SC not only can provide people with the continuous contraception care they need and desire, but also limit the risks of COVID-19 spread.
Members of the Reproductive Health Access Network are taking a stand against these access barriers and are organizing in their states, like California and New York, to pressure policymakers to guarantee coverage of DMPA-SC during COVID-19, and beyond. For example, in March as COVID-19 cases in the US began to grow, Dr. Jennifer Karlin, a family physician and family planning fellow at the University of California San Francisco, contacted Medi-Cal (the public health insurance provider in California) to advocate for coverage of self-administered DMPA-SC. The Chief Policy Officer (CPO) for the Pharmacy Policy Division within Medi-Cal reached out to Dr. Karlin and requested an informal literature review on the safety and efficacy of self-administration. This advocacy and literature review provided evidence for Medi-Cal to pass a temporary policy on April 8, 2020 to pay for pharmacy-dispensed DMPA-SC without requiring prior approval. Dr. Karlin explained:
“By aligning the State of California’s goals of social distancing and maintaining access to the drug benefit with the goals of expanding access to contraceptives based on patient preference, we were actually able to facilitate reproductive autonomy in the State of California during a health care emergency.”
But Dr. Karlin is not done. As Medi-Cal passed a temporary policy, she and the CPO hope to analyze Medi-Cal claims data about usage, continuation, and outcomes during this coverage expansion, as well as interview patients regarding their interest and experiences switching from the clinic-administered intramuscular injection to self-administered DMPA-SC. Such data may support continued state-based and national advocacy efforts for expanding coverage of DMPA-SC after the pandemic.
To support ongoing advocacy, RHAP has been working to understand the national scope of DMPA-SC insurance coverage and pharmacy availability. By exploring various insurance plan formularies online, we found differences in coverage across companies. But, if a company covers DMPA-SC in one state, they likely cover it in all states. Some plans require co-pays and/or prior authorization, but others cover it fully under the Affordable Care Act. Some did not cover DMPA-SC at all. Additionally, RHAP volunteers have been calling a random selection of franchise and community pharmacies in various states to investigate the availability of DMPA-SC and pharmacists’ awareness of this contraceptive method. Among 76 pharmacies called in states like New York, New Jersey, California, Illinois, Alabama, Connecticut, Indiana, Louisiana, and Iowa, we found that most pharmacists were unfamiliar with DMPA-SC. 60% of pharmacies called would dispense DMPA-SC, but it would take 24-48 hours to fill as they would have to order the medication. However, a few stated they would only fill the prescription if a doctor called to confirm that the patient can self-administer. Nearly all pharmacies called in Alabama and Iowa would not dispense DMPA-SC.
The fight to increase access to DMPA-SC during and after the pandemic continues. While advocating for temporary coverage in individual states may be a faster solution, to truly strengthen access during and after the pandemic, national-level advocacy is required. This includes a plan to change the DMPA-SC label to include self-administration. If you are a clinician and would like to share stories regarding patients who have wanted to switch to DMPA-SC from the intramuscular version, and whether they have been able to do so, please contact RHAP’s Research and Evaluation Manager at silpa@reproductiveaccess.org. To learn more about DMPA-SC as a method of contraception, check out RHAP’s resources and Innovating Education’s video “This is How I Teach: Self-Injection DMPA-SC” (narrated by Dr. Karlin).

At RHAP we’re constantly updating and developing new resources to meet the needs of patients, clinicians, and the public. It is important to us that our work, including the resources we create, reflect our values of being evidence-based and patient-centered. One way we keep our resources aligned to our values is by getting input from our wider RHAP community. We currently have two opportunities for our supporters to get involved and provide us feedback.
We’ve developed a new Fact Sheet on How to Use Abortion Pills. This sheet includes both written guidance and helpful images. We are looking for non-clinicians to help us review this new fact sheet and provide us with feedback. We will send out our adorable RHAP tote bags to the first ten people to submit their feedback. If you would be interested in helping us make this resource as useful and accessible as possible, you can access the feedback form here.
Last year we released the Sam’s Medication Abortion zine, which follows one person’s experience of a medication abortion. We’ve translated this zine into Spanish, but we need your help to make sure it’s perfect. We’re looking for a few fluent Spanish speakers to review the translation we’ve done for this zine and to provide us with feedback on any vocabulary and grammar edits we might need to make. We will provide reviewers with a $100 honorarium for their feedback. If you are interested in helping us with this project, please email our Program Manager, Jordan Silverman, at jordan@reproductiveaccess.org.

This summer, we are thrilled to have Vishu Chandrasekhar as our full-time summer intern! Vishu matched with us through the Reproductive Rights Activist Service Corps (RRASC) and, due to the COVID-19 pandemic, is our first fully virtual intern. Learn more about Vishu below and find out how you too can join our team this fall.
Vishu Chandrasekhar is a rising sophomore studying political science and sociology at Case Western Reserve University (CWRU). She is very excited to join RHAP as an intern. She’s passionate about dismantling the racial injustices in our health system and making reproductive care accessible and inclusive for all. Vishu’s serves on the executive board of the Undergraduate Diversity Collaborative and CWRU Mock Trial, is a Social Justice Institute Scholar, and a facilitator for the Emerging Leaders Program. Vishu also enjoys sneakers, comic books, and pursuing the elusive goal of completing the Saturday New York Times crossword.
Welcome, Vishu!
Due to the ongoing pandemic, our fall Development Intern will be remote for the first time as well. If you or someone you know is interested in learning more about fundraising for reproductive health care access, apply to join our team!
The past few months have been a time of national reckoning. The COVID-19 pandemic has exposed long-standing disparities in our health care system, and politicians have used this time of crisis to further restrict reproductive access. The Black Lives Matter movement and the current uprising against white supremacy have reminded us that we, as a country, have a long way to go in order to dismantle white supremacy and existing systems of oppression. At RHAP, we are committed to learning from organizers in the Reproductive Justice movement and incorporating reproductive justice principles in our fight for reproductive health access for all. We recognize that reproductive freedom cannot be achieved without addressing the institutional racism within our healthcare system, and we are in solidarity with the Black Lives Matter movement, Black colleagues, protestors, and organizers who are condemning anti-Black racism and state-sanctioned violence. In our official statement, we’ve outlined an action plan for incorporating a racial justice lens into our work and centering the voices of Black, Indigenous, People of Color (BIPOC).
We have also heard decisions by the Supreme Court, with vast repercussions for reproductive access throughout the country. One such ruling was June Medical v. Russo, where the Court followed precedent from Whole Woman’s Health v Hellerstedt and struck down a medically unnecessary admitting privileges law in Louisiana. We celebrated this victory, while recognizing that it did not protect abortion access definitively or make abortion more accessible to the millions of people throughout the country still denied reproductive and bodily autonomy. In Trump v Pennsylvania, the Court sided with the Trump administration and let employers with religious or moral objections limit birth control access under the Affordable Care Act, resulting in thousands of people losing contraceptive coverage. We condemned this ruling as part of the government’s constant attack on reproductive freedom, especially despicable within the context of the pandemic.
In light of all of these developments, one thing stays constant: we pledge to continue our fight to make reproductive health care accessible to all.
Read our full statements here:
This article was written by our summer intern, Vishu Chandrasekhar. Vishu is supported by the Civil Liberties and Public Policy Program.
Your gift allows us to train and support health care providers across the United States so they can offer patients compassionate and comprehensive care.
Aug 14