Aug 14

Help Us Protect Access to Sexual and Reproductive Health Care Today!
 The mission of the Reproductive Health Access Project (RHAP) is to expand and protect access to reproductive health care for everyone – this includes people of all gender identities and expressions. For us, expanding and protecting access means ensuring clinicians have the training and resources to best serve the reproductive health needs of their entire community. This means that patients of all genders must have clinicians they can trust for their health care, as well as legal protection against discrimination. The transgender, gender non-conforming, intersex, and non-binary communities already face significant barriers in receiving unbiased, patient-centered, and safe reproductive health care. The memo that was published detailing the Trump administration’s proposal to narrowly define gender based on genitalia at birth further threatens the safety, well-being, and access to quality health care for the transgender, gender non-conforming, intersex, and non-binary patients our clinicians serve. If passed, this regulation would change the legal definition of gender, effectively legalizing the discrimination against and the erasure of non-binary people.
The mission of the Reproductive Health Access Project (RHAP) is to expand and protect access to reproductive health care for everyone – this includes people of all gender identities and expressions. For us, expanding and protecting access means ensuring clinicians have the training and resources to best serve the reproductive health needs of their entire community. This means that patients of all genders must have clinicians they can trust for their health care, as well as legal protection against discrimination. The transgender, gender non-conforming, intersex, and non-binary communities already face significant barriers in receiving unbiased, patient-centered, and safe reproductive health care. The memo that was published detailing the Trump administration’s proposal to narrowly define gender based on genitalia at birth further threatens the safety, well-being, and access to quality health care for the transgender, gender non-conforming, intersex, and non-binary patients our clinicians serve. If passed, this regulation would change the legal definition of gender, effectively legalizing the discrimination against and the erasure of non-binary people.
RHAP stands in solidarity with our transgender, gender non-conforming, intersex, and non-binary communities and will continue our fight to protect and expand access to reproductive health care that is affirming for all people. For ways to take action on this, please check out this article from OUT magazine.
With the RHAP team the largest that it has ever been, we have brought on three new interns for the fall to provide key support on our ongoing Development, Communications, and Programmatic initiatives. We are thrilled to introduce these new team members who will help us continue to work towards making comprehensive reproductive health care accessible to everyone. Get to know our new interns below:
Rebecca Schwarz, Communications Intern
 Becca is a graduate of Wellesley College, where she earned her BA in Sociology and dabbled with a minor in Economics. Before coming to RHAP, she worked in health care public relations (PR) for two years as an account executive at a global health care communications agency, providing PR support to a wide range of pharmaceutical companies. While working in PR, Becca kept returning to her original interests in reproductive rights, health, and access, and has since come to RHAP to flex her communications muscles for the team! When she’s not in the office working with Hailey to manage and boost RHAP’s social media channels, Becca is working on applications to return to school next fall with the goal of earning her MPH – fingers crossed!
Becca is a graduate of Wellesley College, where she earned her BA in Sociology and dabbled with a minor in Economics. Before coming to RHAP, she worked in health care public relations (PR) for two years as an account executive at a global health care communications agency, providing PR support to a wide range of pharmaceutical companies. While working in PR, Becca kept returning to her original interests in reproductive rights, health, and access, and has since come to RHAP to flex her communications muscles for the team! When she’s not in the office working with Hailey to manage and boost RHAP’s social media channels, Becca is working on applications to return to school next fall with the goal of earning her MPH – fingers crossed!
What do you like to do in your spare time?
I love working out and spending time with my friends – ideally doing both at the same time! I also do the New York Times crossword every morning in the hope that someday I’ll be able to do the full set of weekly puzzles without anyone’s help.
What is a fun fact about yourself?
I’m a boomerang intern at RHAP – I first worked here during the summer of 2014, and I loved the team and the mission so much that I couldn’t help but come back!
What is one of your favorite reads on Reproductive Justice/Reproductive Health/Reproductive Rights?
The Story of Jane: The Legendary Underground Feminist Abortion Service by Laura Kaplan
Jaci Deitch, Program Intern
Reproductive justice has always had a significant place in Jaci’s life, and she is thrilled to be fulfilling that passion by working with RHAP. Jaci is currently working independently as a communications consultant for a centrist media platform, advising on messaging strategies and discussion topics that convey social justice principles. She is primarily interested in domestic reproductive health policy and law, as well as increasing access to comprehensive patient-centered care. Jaci earned her MPH from Columbia University with an emphasis in sexual and reproductive health and has previously worked with the UN Population Division, St. James Infirmary, and San Francisco Sex Information.
What do you like to do in your spare time?
Practice Pilates, dance, and travel.
What is a fun fact about yourself?
I’ve lived in four different coastal cities on three different continents.
What is one of your favorite reads on Reproductive Justice/Reproductive Health/Reproductive Rights?
Hard to say what my favorite is, but I love Rickie Solinger’s work; Pregnancy and Power and Reproductive Justice: An Introduction with Loretta Ross (whose work is also amazing!) are must-reads for any reproductive justice advocate.
Alison Silverstein, Development Intern
 Alison graduated with her BA in Romance Studies, a joint study of French and Spanish language and literature, from Wesleyan University. At Wesleyan, she joined and became coordinator of Clinic Escorts, a student group which supports the last independent clinic in Connecticut with escort volunteers. Additionally, the student group provided support for pro-choice legislation through their partnership with NARAL Pro-Choice Connecticut. With help from escort testimonials, Hartford passed an ordinance that bans Crisis Pregnancy Centers from disseminating false information about the services they provide. Since college, Alison has taken an interest in the non-profit world and has worked with City Lore and the Brooklyn Academy of Music (BAM).
Alison graduated with her BA in Romance Studies, a joint study of French and Spanish language and literature, from Wesleyan University. At Wesleyan, she joined and became coordinator of Clinic Escorts, a student group which supports the last independent clinic in Connecticut with escort volunteers. Additionally, the student group provided support for pro-choice legislation through their partnership with NARAL Pro-Choice Connecticut. With help from escort testimonials, Hartford passed an ordinance that bans Crisis Pregnancy Centers from disseminating false information about the services they provide. Since college, Alison has taken an interest in the non-profit world and has worked with City Lore and the Brooklyn Academy of Music (BAM).
What do you like to do in your spare time?
I like to cook elaborate meals and read.
What is a fun fact about yourself?
I had an essay published in the Queens Tribune at the age of 10 about how great my mom was. She got to go on the field at Shea Stadium to receive a Best Mom award!
What is one of your favorite reads on Reproductive Justice/Reproductive Health/Reproductive Rights?
Our Bodies, Our Crimes: The Policing of Women’s Reproduction in America by Jeanne Flavin
 Did you know that it costs $90 to purchase the two types of pills (mifepristone and misoprostol) used for a medication abortion? Mark your calendars and join RHAP on November 27th for #GivingTuesday. We are looking to provide start-up supplies to the clinicians we train so that they can start integrating medication abortion care into their practice. All proceeds raised on this day will be matched 2 for 1, up to $6000, and will go towards expanding access to medication abortion. Donate on #GivingTuesday! #AbortionAccess is #InYourHands.
Did you know that it costs $90 to purchase the two types of pills (mifepristone and misoprostol) used for a medication abortion? Mark your calendars and join RHAP on November 27th for #GivingTuesday. We are looking to provide start-up supplies to the clinicians we train so that they can start integrating medication abortion care into their practice. All proceeds raised on this day will be matched 2 for 1, up to $6000, and will go towards expanding access to medication abortion. Donate on #GivingTuesday! #AbortionAccess is #InYourHands.
 November was declared Native American Heritage Month in 1990. However, the fight for the celebration and national recognition of Native Americans’ and Alaskan Natives’ history, culture, and traditions began decades beforehand. Dr. Arthur C. Parker, historian and member of the Seneca Nation, was one of the early proponents of “American Indian Day.” During the early 1900s, he convinced the Boy Scouts of America to designate a day for the “First Americans.” For centuries, Native American and Alaskan Native activists have fought against colonial erasure and have mobilized to preserve their history, traditions, and autonomy. Central to this fight is defending the reproductive freedom of Native American and Alaskan Native Communities.
November was declared Native American Heritage Month in 1990. However, the fight for the celebration and national recognition of Native Americans’ and Alaskan Natives’ history, culture, and traditions began decades beforehand. Dr. Arthur C. Parker, historian and member of the Seneca Nation, was one of the early proponents of “American Indian Day.” During the early 1900s, he convinced the Boy Scouts of America to designate a day for the “First Americans.” For centuries, Native American and Alaskan Native activists have fought against colonial erasure and have mobilized to preserve their history, traditions, and autonomy. Central to this fight is defending the reproductive freedom of Native American and Alaskan Native Communities.
Systemic poverty and lack of access to quality health care disproportionally affect Alaska Natives and Native Americans. Per the CDC, “…nationwide, American Indian and Alaska Native infants are nearly twice as likely to die by their first birthday as non-Hispanic white infants.” [1] The rate of Sexually Transmitted Diseases amongst Alaska Native and Native American youth is one of the highest in the county.[2] Limited community-based research on the reproductive health needs of geographically and culturally diverse Alaska Native and Native American populations contributes to inadequate reproductive health services that do not meet the needs of indigenous communities.
This month, the Reproductive Health Access Project is proud to highlight indigenous activists combating reproductive oppression within the movement in our year-long reproductive justice campaign, “A Common Thread: Weaving Reproductive Health, Rights, and Justice.” You will get to read more about trailblazers like women’s health advocate and renowned coalition builder, Charon Asetoyer, who established the Native American Women’s Health Education Resource Center – a non-profit that focuses on several initiatives including cultural preservation, indigenous reproductive rights, and community-based research on Native American health needs. Additionally, you will learn more about activists like Madonna Thunder Hawk, co-founder of Women of All Red Nations, an organization that advocated for indigenous women forcibly sterilized, fought for indigenous land restoration, and highlighted the detrimental effects of environmental racism on Native Americans’ health.
 It has been a busy fall for our Reproductive Health Access Network! In addition to hosting Cluster meetings in almost all of our states, our Network members have been engaging in more advocacy than ever before.
It has been a busy fall for our Reproductive Health Access Network! In addition to hosting Cluster meetings in almost all of our states, our Network members have been engaging in more advocacy than ever before.
In early October, at this year’s American Academy of Family Physician’s (AAFP) Congress of Delegates (the governing body of the organization, with a structure that is similar to the U.S. Senate) a group of nearly 30 Network leaders gathered in New Orleans and successfully advocated for the passage of four reproductive health resolutions:
– Resolution 408: Reduce maternal mortality
– Resolution 506: Removing REMS categorization on Mifepristone
– Resolution 507: Oppose the criminalization of self-induced abortion
– Resolution 509: Opposed fetal personhood terminology in governmental policies and legislation
Network advocates also successfully opposed Resolution 508: “Elective Abortions,” which urged the AAFP to support 20-week abortion bans. Engaging in advocacy efforts within the AAFP is a powerful way for our members to use their voices as clinicians to encourage their professional organization to take a pro-choice public stance on reproductive health care and access issues.
That same week, AAFP leaders also participated in a daylong community organizing and leadership building training, facilitated by Miriam Yeung, MPA. Miriam is an organizer and longtime reproductive justice advocate, who formerly led the National Asian Pacific American Women’s Forum. Thanks to Miriam, our leaders left the training better equipped to serve as proud advocates for reproductive and abortion care within the AAFP and beyond it.
Later that month, RHAP Network members came together once more at the North American Forum on Family Planning, a national conference of family planning providers, researchers, and advocates from all different disciplines. We hosted a breakfast for 30 of our Cluster leaders, as well as our annual National Network gathering. The turnout this year was higher than ever before – we had 90 clinicians from across the country join us to network and strategize with their colleagues!
The Reproductive Health Access Network is RHAP’s community of over 2,300 primary care clinicians who mobilize to expand access to abortion, contraception, and miscarriage care in their primary care settings. Network members engage in training, advocacy, and peer support both locally and nationally. The Network currently has 21 Clusters, or chapters, of clinicians who engage in Network activities in their local communities. Currently, we have Clusters in 20 states. If you are a clinician and would like to be connected with your local Cluster, or would like to start one in your state, please email Laura Riker, RHAP Senior Program Manager.
 In July of 1981, activists at the first Feminist Encentro for Latin America and the Caribbean declared November 25th the International Day for the Elimination of Violence Against Women. The day was originally selected to honor the Mirabal sisters, three Dominican feminists assassinated in 1960 for defying the Trujillo dictatorship, and to bring international attention to the pervasiveness of gender violence. [1]
In July of 1981, activists at the first Feminist Encentro for Latin America and the Caribbean declared November 25th the International Day for the Elimination of Violence Against Women. The day was originally selected to honor the Mirabal sisters, three Dominican feminists assassinated in 1960 for defying the Trujillo dictatorship, and to bring international attention to the pervasiveness of gender violence. [1]
According to a UN report that gathered data from over 87 countries between 2005 to 2016, “…19 percent of women between 15 and 49 years of age said they had experienced physical and/or sexual violence by an intimate partner in the 12 months prior to the survey.” [2] Ending gender violence is imperative to achieving reproductive freedom. For this year’s International Day for the Elimination of Violence Against Women, RHAP is honored to feature Dr. Anita Ravi’s powerful article, “Advocating for Our Patients in the #MeToo Era.“
This article was originally published as a post in the American Academy of Family Physician’s Fresh Perspectives blog.
“Advocating for Our Patients in the #MeToo Era”
by Anita Ravi, MD, MPH, MSHP, FAAFP | Founder, Medical Director- The PurpLE Clinic at The Institute for Family Health | Assistant Professor- Department of Family Medicine & Community Health, Icahn School of Medicine at Mount Sinai
The burden of fighting the culture of sexual violence does not and cannot lie solely on survivors. It must include the voices of physicians. The 2018 Nobel Peace Prize recipients offer a beautiful example of this dual effort. Denis Mukwege, M.D., Ph.D., and activist Nadia Murad — herself a survivor — were both recognized last week for their efforts to end the use of sexual violence as a weapon of war.
Three years ago, I started what you might call a #MeToo family medicine clinic. The PurpLE Clinic at the Institute for Family Health in New York, N.Y., was designed for people who have experienced sexual trauma, including sexual assault, domestic violence and sex trafficking. Every criticism from the outside world, from “Why didn’t she report it?” to “What if she’s lying?” can be answered inside the clinic. And yet, when I leave the confines of the medical space, I see these questions stubbornly fester in public discourse, exploiting the silence and circumstances of sexual trauma survivors.
As a doctor, I am compelled to counter the harmful misconceptions regarding sexual violence and trauma with truths that I have learned from clinical practice. Here are a few:
Story Telling
My clinical exam room is a graveyard of smashed stereotypes of what some people think victims should be — a distressed individual who provides a linear story with a desire to report the assault immediately.
![]()
Recounting a sexual assault is nonformulaic. Stories may come out as you make contact with the doorknob to leave the exam room, are about to begin a Pap smear, or have just placed a stethoscope on the heart. They may spill out hours after an assault or 20 years later. They may be the reason for a medical visit, or they may unexpectedly come up when you talk about diet and exercise and hear, “I tried to gain weight and stopped wearing makeup so I wouldn’t be raped again.”
As physicians, our responsibility to counter rape culture is not simply to share stories, but to share how our patients share their stories. We must lend credence to the unexpected smiles, inevitable gaps in memory and nonlinear information that is normal in trauma. The first sexual assault exam I ever did was with a teenage girl. She had never had a speculum exam. I asked if anything would make her feel more comfortable. She turned on her iTunes, and we started her exam with music blaring in the background. She had come in with her best friend. They laughed and giggled together. Her assault had occurred just seven hours earlier. That is trauma. Our public awareness must evolve to understand trauma’s permutations so survivors are not wrongly scrutinized.
Photos
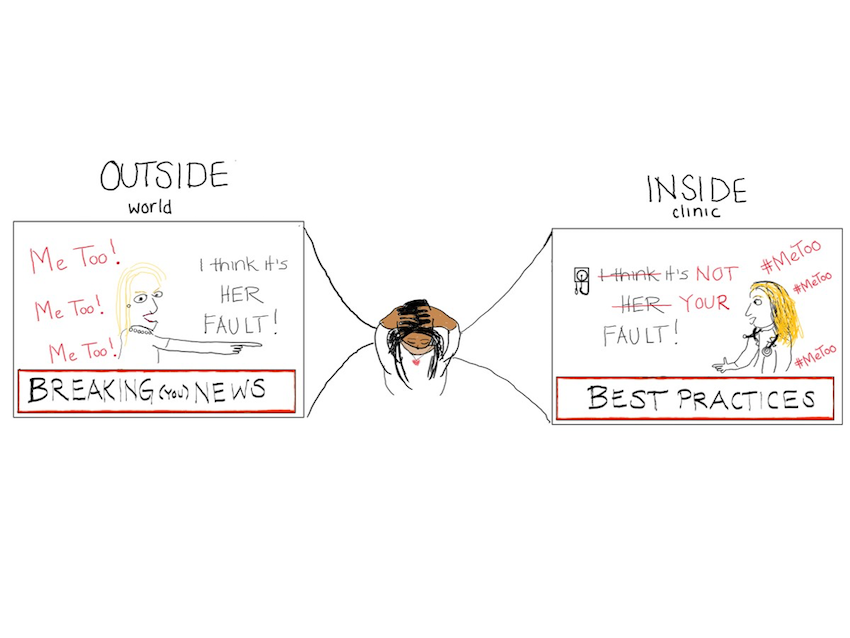
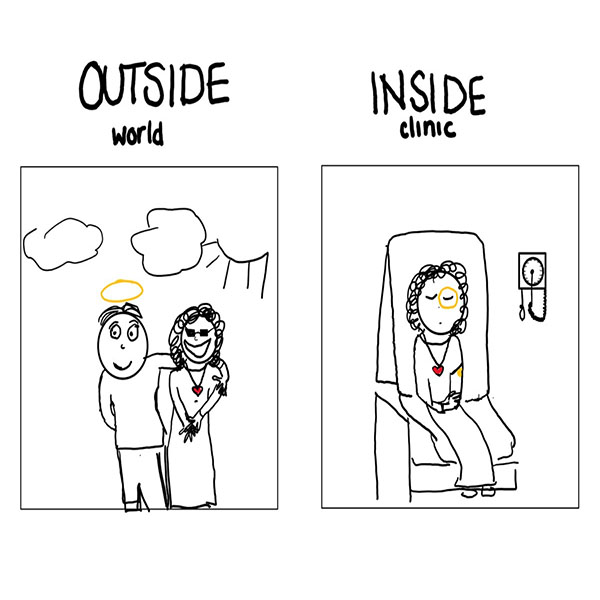
“But they looked so happy” is a common reaction when people learn that someone they know was in an abusive relationship. There are pictures seen by the outside world — images of a healthy, loving relationship, beautifully curated and filtered photos on Facebook and Instagram.
And then there are the photos I take in-clinic. Smiles to the external world are irrelevant in the confines of the exam room.
 Every time I meet someone who has experienced a recent sexual assault or domestic violence, I ask two questions: “Do you plan to file a police report?” and “Would you like photos of the injuries in your medical record?” The answer is almost always “No” to the first and “Yes” to the second.
Every time I meet someone who has experienced a recent sexual assault or domestic violence, I ask two questions: “Do you plan to file a police report?” and “Would you like photos of the injuries in your medical record?” The answer is almost always “No” to the first and “Yes” to the second.
Photographing injuries remains a particularly unnatural and emotionally challenging part of my work. The silence during the 10-second process of setting up the camera always grows uncomfortably large. Sometimes she helps hold the ruler, noting my clumsy efforts to measure the injury while photographing. I press the button. And then I move to the next one. I hope that this process will never feel normal. And I hope that our public consciousness evolves to understand that the presence of happy pictures does not imply an absence of trauma.
Résumés
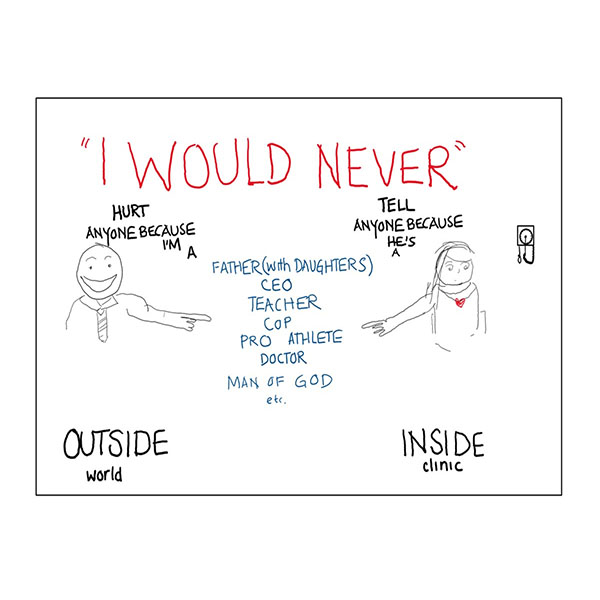
Sexual assault is the abuse of power. It can be power based on many factors: gender, race, sexuality, immigration status, literacy, mental health, and on and on. When an accused person lists an illustrious resume, it tells me about their positions of power, but it does not tell me the responsibility with which they wield it. Being educated or wealthy is not a prophylactic against perpetrating violence. People in highly esteemed positions of power have hurt my patients. It’s a common reason that people don’t report the crime. In cases of sexual assault, résumés are not needed.
Résumés are also often used to highlight the harm to those who are accused of sexual assault. What if it’s not true? A person’s hard-earned standing in the world has been ruined. Look at what they’ve lost.
I wish this remarkable empathy could be applied in understanding the loss that comes with sexual assault. But it’s harder to quantify the loss of opportunities that were never actualized. In medicine, we are taught about “insensible losses” — the loss of fluids from our body that can neither be perceived nor measured directly but are critical to account for. Some sexual assault survivors experience a form of insensible loss on their résumés. The invasion of posttraumatic stress disorder, depression and anxiety following sexual assault can result in life-altering changes that impact career trajectories. These are financial, physical and emotional losses that are masked by survivors’ resilience.
When asked about their dream job, my patients commonly respond, “I used to want to be X, but now I’d rather be Y.” X has included becoming a business owner, social worker or health professional, while Y has frequently included wanting to be a mortician or custodial worker — something quieter “where no one harasses you or tells you, ‘Your ass looks nice.'” These résumé changes often go undetected during the “inconvenience” of sexual assault accusation discussions, but it’s time for them to be accounted for and acted on in our collective response to sexual violence.
Witness
As each day of clinic wraps up and I step outside, two truths stubbornly, persistently demand my attention on my walk home: Sexual violence is a cultural infection, and adding physician voices is necessary for its eradication. Physicians bear witness to the patterns of stories that deserve to influence policies but may never be heard. The shared work of survivors and physician-allies is necessary to change our culture and to secure a future immune to sexual violence.
 Silpa Srinivasulu and Linda Prine both started Facebook birthday fundraising campaigns to benefit the Reproductive Health Access Project, asking their friends to support us for their birthdays! Together they raised a total of $2,161 for RHAP. Thank you Silpa and Linda!!!
Silpa Srinivasulu and Linda Prine both started Facebook birthday fundraising campaigns to benefit the Reproductive Health Access Project, asking their friends to support us for their birthdays! Together they raised a total of $2,161 for RHAP. Thank you Silpa and Linda!!!
Would you like to fundraise for RHAP? We just launched our own tools so that you have a simple, do-it-yourself way of supporting us. Use your creativity and passion to take an active role by fundraising and spreading awareness about access to reproductive health care. If you’d like to start a birthday fundraiser for RHAP, fundraise in your community, workplace, or in other ways, click here and start fundraising today!
Your gift allows us to train and support health care providers across the United States so they can offer patients compassionate and comprehensive care.
Aug 14