Language in the Exam Room
 The medical students and residents we train are often surprised at the emphasis we put on language in the exam room. Take this recent story from a family doctor in our practice who was working with a medical student:
The medical students and residents we train are often surprised at the emphasis we put on language in the exam room. Take this recent story from a family doctor in our practice who was working with a medical student:
While examining the patient she [the medical student] used phrases like, “Scoot your bottom down until you feel like you are about to fall off” and “You are going to feel me clean your cervix now.” I knew that the medical student was patient-centered but that wasn’t coming across in the words she was using. At the end of day, the student and I brainstormed some ways she could improve her use of language. Since no one wants to feel like they are about to fall off the exam table, we decided to instead say “There is more room on the table for you to slide down towards me.” We also thought that using the word clean implies that we think the vagina is dirty, so instead we could say “You are going to feel some cool wet gauze now.”
This training story is a great example of how our language can affect our patients. It feels really different to women who come in with an unintended pregnancy to be asked, “Do you want to be pregnant?” rather than, “Do you want to keep your baby?” The judgment implied in keeping your baby is harsh. What else would you do? Throw it out? Get rid of it? Yet these terms are so common that I have even had women tell me, “I can’t be pregnant now, I need to get rid of it.”
Sadly, women absorb the shame our society places on them if they want to end a pregnancy. It is important for us, as health care providers, to use language carefully. Our language in the exam room should reflect the respect we feel for our patients and for their decisions. Professionally, we want to use language that cannot be construed in any way to be sexual. So, we tell women during the exam “Everything looks healthy and normal,” not “Everything looks good.” We call the exam table a table and not a bed.
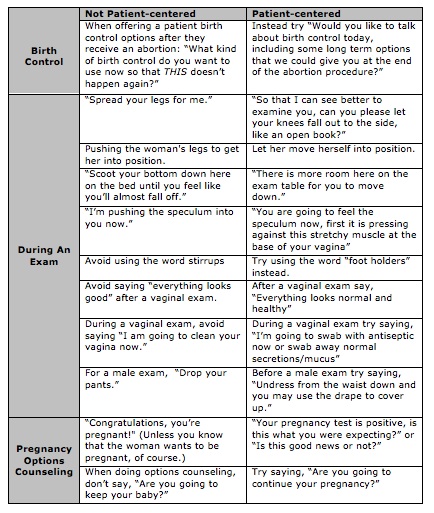
With a group of family medicine residents, we had a further brainstorming session about language, remembering some of the worst things we’d all heard over the years, and came up with better alternatives. The table in this blog post is our summary. We know many conscientious clinicians and health care workers mull over the best use of language to make patients comfortable. We’d love to hear from you about other examples language – both good and bad.

{kind=link}